


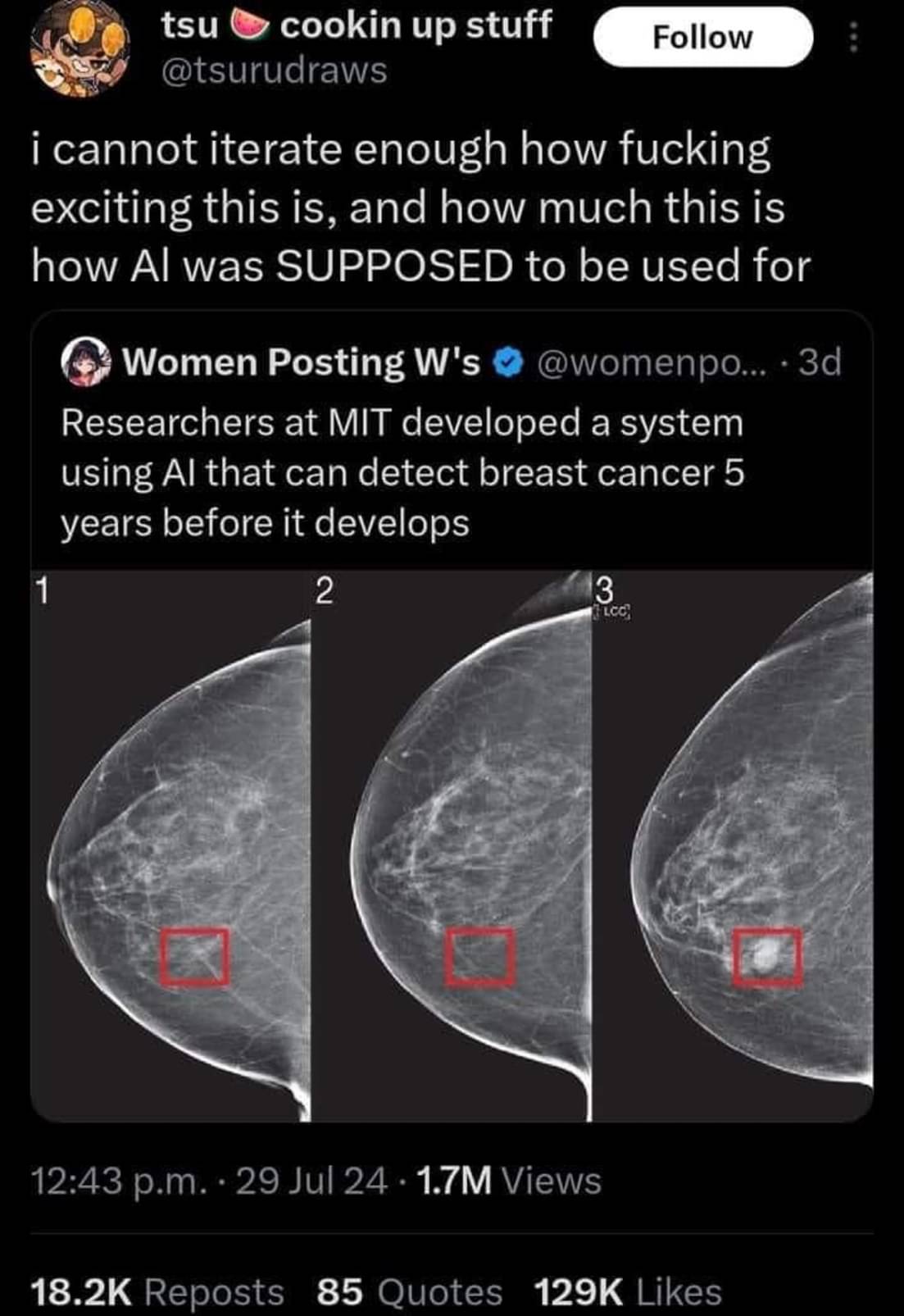
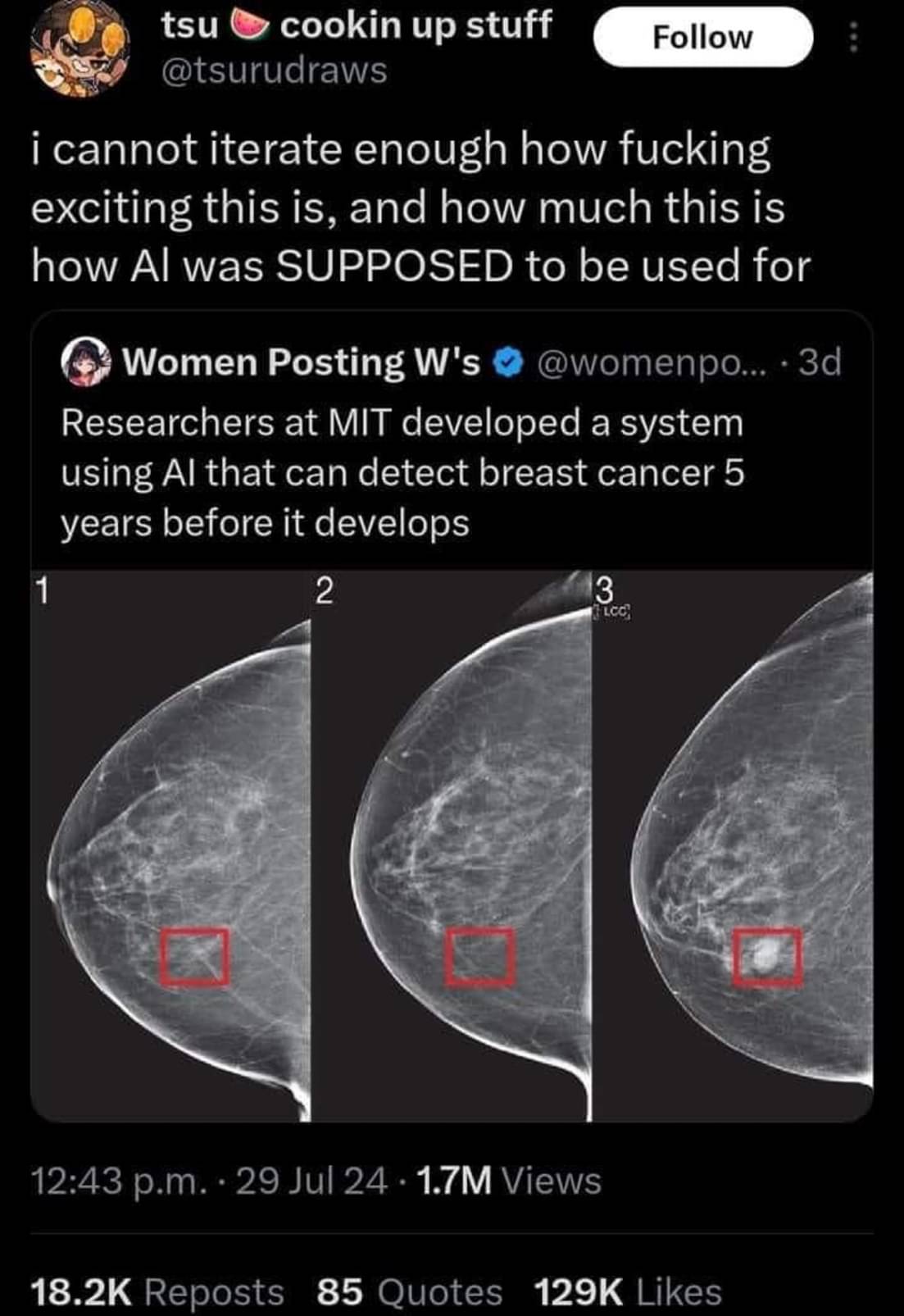
Unfortunately AI models like this one often never make it to the clinic. The model could be impressive enough to identify 100% of cases that will develop breast cancer. However if it has a false positive rate of say 5% it’s use may actually create more harm than it intends to prevent.

Another big thing to note, we recently had a different but VERY similar headline about finding typhoid early and was able to point it out more accurately than doctors could.
But when they examined the AI to see what it was doing, it turns out that it was weighing the specs of the machine being used to do the scan… An older machine means the area was likely poorer and therefore more likely to have typhoid. The AI wasn’t pointing out if someone had Typhoid it was just telling you if they were in a rich area or not.
That’s actually really smart. But that info wasn’t given to doctors examining the scan, so it’s not a fair comparison. It’s a valid diagnostic technique to focus on the particular problems in the local area.
“When you hear hoofbeats, think horses not zebras” (outside of Africa)
AI is weird. It may not have been given the information explicitly. Instead it could be an artifact in the scan itself due to the different equipment. Like if one scan was lower resolution than the others but you resized all of the scans to be the same size as the lowest one the AI might be picking up on the resizing artifacts which are not present in the lower resolution one.
That is quite a statement that it still had a better detection rate than doctors.
What is more important, save life or not offend people?
The thing is tho… It has a better detection rate ON THE SAMPLES THEY HAD but because it wasn’t actually detecting anything other than wealth there was no way for them to trust it would stay accurate.
Not at all, in this case.
A false positive of even 50% can mean telling the patient “they are at a higher risk of developing breast cancer and should get screened every 6 months instead of every year for the next 5 years”.
Keep in mind that women have about a 12% chance of getting breast cancer at some point in their lives. During the highest risk years its a 2 percent chamce per year, so a machine with a 50% false positive for a 5 year prediction would still only be telling like 15% of women to be screened more often.
Breast imaging already relys on a high false positive rate. False positives are way better than false negatives in this case.
That’s just not generally true. Mammograms are usually only recommended to women over 40. That’s because the rates of breast cancer in women under 40 are low enough that testing them would cause more harm than good thanks in part to the problem of false positives.
Nearly 4 out of 5 that progress to biopsy are benign. Nearly 4 times that are called for additional evaluation. The false positives are quite high compared to other imaging. It is designed that way, to decrease the chances of a false negative.

How would a false positive create more harm? Isn’t it better to cast a wide net and detect more possible cases? Then false negatives are the ones that worry me the most.
It’s a common problem in diagnostics and it’s why mammograms aren’t recommended to women under 40.
Let’s say you have 10,000 patients. 10 have cancer or a precancerous lesion. Your test may be able to identify all 10 of those patients. However, if it has a false positive rate of 5% that’s around 500 patients who will now get biopsies and potentially surgery that they don’t actually need. Those follow up procedures carry their own risks and harms for those 500 patients. In total, that harm may outweigh the benefit of an earlier diagnosis in those 10 patients who have cancer.
Well it’d certainly benefit the medical industry. They’d be saddling tons of patients with surgeries, chemotherapy, mastectomy, and other treatments, “because doctor-GPT said so.”
But imagine being a patient getting physically and emotionally altered, plunged into irrecoverable debt, distressing your family, and it all being a whoopsy by some black-box software.
That’s a good point, that it could burden the system, but why would you ever put someone on chemotherapy for the model described in the paper? It seems more like it could burden the system by increasing the number of patients doing more frequent screening. Someone has to pay for all those docter-patient and meeting hours for sure. But the benefit outweighs this cost (which in my opinion is good and cheap since it prevents future treatment at later stages that are expensive).


{kind=link}
{kind=link}